

Biceps Tendinosis
If you are suffering from pain in the front of your shoulder, you may be experiencing biceps tendinosis. Biceps tendinosis can be difficult to diagnose and is often confused with rotator cuff tendinosis and bursitis. At Nebraska Hand & Shoulder Institute, you can trust our expert staff to properly diagnose your shoulder pain and provide the best treatment plan for your condition. Contact us today to schedule an appointment for your shoulder pain.
Understanding Biceps Tendinosis
Biceps tendinosis is very hard to confirm. Overall, I think the biceps tendon has been over-emphasized in the past decade with the main problems overall being the painful arc syndrome with a prominent acromion necessitating acromioplasty in those patients who continue to complain of pain not responding to NSAIDs or activity change. Pain in front of a person’s shoulder (anterior) is the hallmark symptom. It usually occur with elevation of the arm forward, i.e. flexion, however, this is the position that most patients hurt with bone impingement from a prominent acromion. Therefore it is difficult to differentiate rotator cuff tendinosis and bursitis from biceps tendinosis.
The long head of the biceps tendon (LHBT) originates in the top of the glenoid where it attaches with the glenoid labrum. It exits the shoulder joint through the bicipital groove, or bony canal, and is usually not part of the problem, though in old patients it may contribute. It is held in place by the small transverse humeral ligament and then transitions into the biceps muscle. Biceps tendon pain can occur as a result of a recent trauma when the transverse ligament is disrupted resulting in dislocation of the tendon, which is quite rare. Usually pain from biceps tendinosis is related to advanced age, activity, and being pinched by a prominent acromion as part of the “painful arc syndrome” and often in association with a large, chronic rotator cuff tear. In a person over the age of 60 the biceps tendon is often found to be ruptured and scarred in the bicipital groove. An isolated tear of the long head of the biceps tendon (LHBT) may be treated with medication until inflammation and pain go away. If a Popeye deformity is acceptable to the patient, there is no functional loss that results. Persistent pain from a non-ruptured biceps can only be accurately diagnosed with arthroscopy, i.e. the surgeon needs to be prepared to treat a partial or full-thickness tear of the rotator cuff, and biceps pathology as determined by the intraoperative findings.
The two main treatments for biceps tendinosis: 1) Tenodesis; anchoring it in a hole in the humeral neck with a screw or 2) tenotomy, which means to cut the tendon which may lead to a Popeye deformity depending on the contour of the person’s arm. If the biceps tendon is frayed 30% or less, trimming it and performing and acromioplasty, i.e. trimming the prominent acromion, usually gives excellent relief of pain. If fraying beyond 30% it makes the most sense to release the tendon completely and anchor it in the bone, i.e. perform a tenodesis. Tenodesis and tenotomy are also important for pain resulting from damage to the biceps labral complex, i.e. partial pulling away of the biceps and labrum from their attachment in the bone of the glenoid. In patients over the age of 40 research shows this is best treated by tenotomy or tenodesis since repair in this age group is more likely to lead to scarring and stiffness and ongoing problems with pain.

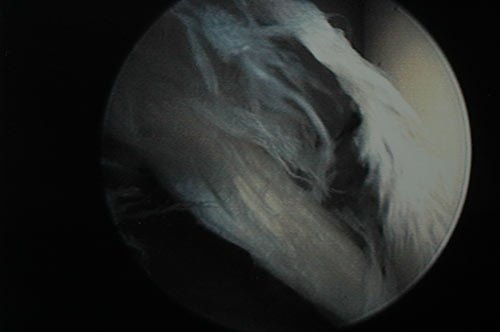
Severe Biceps Tendonitis

50% of bicep rotten

MRI of Bicep Tendonopathy
Shredded bicep
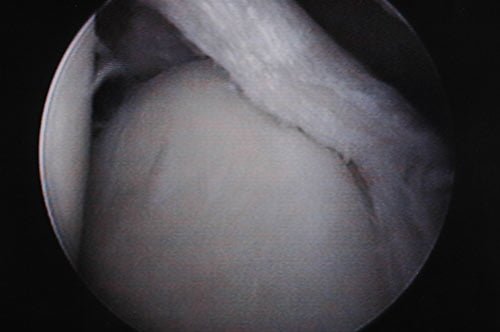
Trimmed bicep

Trimmed bicep

Decayed bicep