

Wrist Fractures
When you experience a broken wrist, you need you expert care in order to avoid long-term consequences. In some situations, proper treatment of a broken wrist can help avoid long-term consequences such as carpal tunnel syndrome. Don't trust the future of your wrist to just anyone, trust the experts at Nebraska Hand & Shoulder.
Understanding Wrist Fractures
A broken bone is known as a fracture. Fractures are graded in their magnitude. One of the most common bones to be broken in the human body is the radius, which is one of the main bones of the wrist. The radius is one of two bones of the forearm ending at the wrist and when it breaks there is a great chance of it breaking into the joint space itself. If this happens, the alignment of the bone must be restored to within 2 mm of normal to avoid arthritis. Whether the bone breaks into the joint or the break is completely outside of the joint, there can still be a deformity. When the bone is broken as a child there is great capacity for spontaneous correction via the process of laying down cartilage which is later converted to bone otherwise known as remodeling. In an adult bone there is little chance of remodeling; what you see is what you get in terms of alignment.

Scaphoid Fractures

Scaphoid Fractures
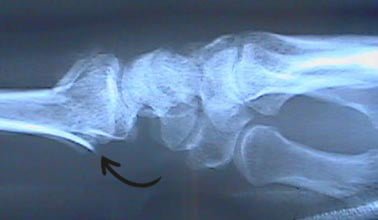
Distal Radius Fracture
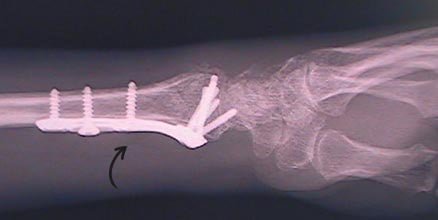
After Plate & Screw Repair
Displaced bones can be pushed back into alignment with a combination of manipulation of the broken bone with the person asleep or with the wrist numb and then it can be reinforced with plaster splint or cast.
In the case of cast treatment, it is usually wise to check x-rays once a week for about three weeks. The earlier a displaced fracture is caught the easier it is to restore the alignment via surgery and correct it. Neither all fractures treated in a cast nor all fractures treated operatively heal perfectly. Some with perfectly restored wrists go on to have stiffness and arthritis.
Some people who break a wrist go on to develop carpal tunnel syndrome. Some of these may have had the makings of carpal tunnel syndrome beforehand, but only become aware of it after the trauma; others have enough scarring and swelling and healing with extra bone to change the carpal canal space and increase pressure on the median and ulnar nerves resulting in abnormal sensation and possibly pain. Nerve conduction study will confirm if these people developed carpal tunnel syndrome. We often talk about the pendulum swinging in the way care is rendered. Trends occur and sometimes they reverse. Over the last decade to decade and a half there has been a trend towards operative reduction and fixation of broken radius fractures using plate-and-screw technique. Some of us still get excellent results when necessary using what is known as an external fixator. Though I use both techniques, they are interchangeable depending on the situation.
There are numerous types of plates for the top and bottom of the wrist, for small and large bone fragments, etc. There are a number of different types of external fixators- a variety of shapes, sizes and weight. There are still a percentage of people who will be quite satisfactorily treated with a cast or splint. The goal is to get the person’s bone to heal as anatomically correct as possible and avoid pain, stiffness, ultimate arthritis or deformity. The healing of a broken bone takes about three weeks to become comfortable, six weeks to become stable and not require external protection, and over three months for complete biologic union. At the time of injury, a person’s bone may be compressed down much like a honeycomb. We try and stretch it out into alignment whether done closed in a cast or operatively with a plate and screws. Depending on the circumstances, it may be advisable to insert some bone taken either from elsewhere in the person’s body or from bone bank from donors that are healthy until they died unexpectedly and gave their parts of their body away to benefit others. This is known as allograft. It is used to support the honeycomb that doesn’t stretch right back like an accordion but rather compact them.
Fractures in Children
If a child breaks his wrist, he typically does so differently than an adult. There is a growth plate at the cartilage-bone junction which is the weakest point. It is here where the child will most often break and we try and restore this close to normal, though it is not absolutely essential as long as the fracture does not actually go through the joint itself. The overwhelming majority are treated nonoperatively by pushing the bone back into place with cast immobilization, sometimes a pin through the skin to hold the bone in place is used in children, and only rarely is open reduction and fixation with a plate and screws or similar ever necessary.
Risks of Surgery
The risk of any surgery always includes infection. The risk is quite small with use of good hygiene, i.e. good sterile technique. The risk gets considerably increased if the person comes in having an open fracture, meaning the bone penetrated through the skin at the time of injury. These need to be washed out to lower the infection risk. Sometimes it is necessary to leave the wound open if it occurred in a very dirty setting and come back days later to close the wound.
Nerve injury can occur in the form of direct median or ulnar nerve bruise at the wrist, when a broken bone or sharp edge points into the nerve. It is extremely unlikely that permanent nerve damage will occur. After trauma with changing the shape of the canal, callus from the healing fracture, may lead to carpal and/or ulnar tunnel syndrome. Failure to heal, known as non-union, can occur in an unhealthy person but it is pretty rare unless she is a smoker. For non-union the surgeon has to consider opening up the fracture site and place some bone graft, then prolonged immobilization with a cast or plate and screws is required.
Mal-union or healing of bone in the improper position, bone shortening, angulation, dorsal or palmar, are recognized risks of radius fractures at the wrists. Our society has become less and less tolerant of deformity, though some people are more concerned about keeping the cost at a minimum then they are about function and appearance. One will occasionally still have a person unwilling to proceed with surgery even when she is going to end up with a definite malunion.